
The knee consists of two major joints: the tibiofemoral joint – the main hinge joint of the knee, and the patellofemoral joint – which acts as a pulley mechanism to allow for the smooth transition of knee extension to flexion. To achieve this, the patella (kneecap) sits in a groove in the femur (thigh bone), which is covered in cartilage. The patella glides over this cartilage whenever the knee moves.
Injury mechanics:
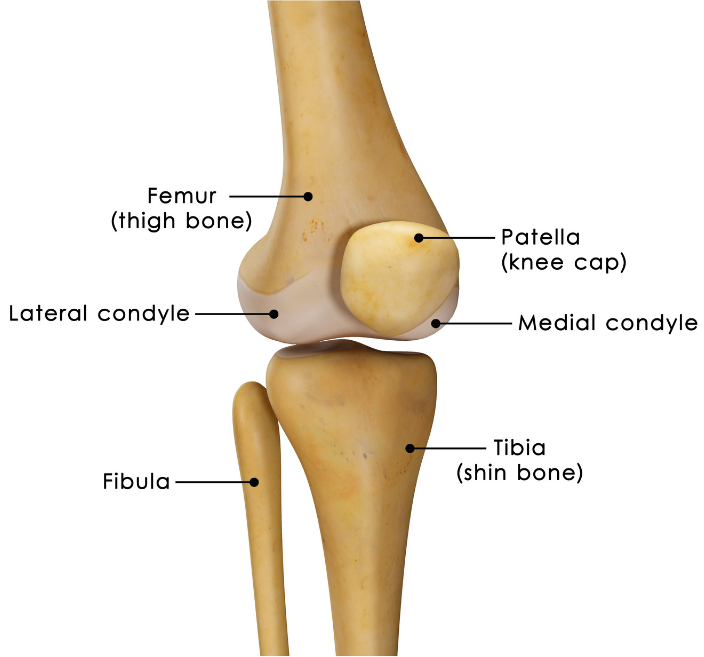
Altered tracking of the patella during knee flexion and extension due to biomechanical changes often results in pain around the knee. This is due to a change in the directional forces applied to the patella on movement. These changes cause the patella to shift out of the groove and apply pressure to the femoral condyles (the bony prominences beside the femoral groove) and thus can cause overuse/overload (overpressure) on that part of the femur. The pressure can result in pain, discomfort or irritation and eventually contributes to damage of the cartilage surfaces. This is called Patellofemoral Pain Syndrome (PFPS).
PFPS can occur as a result of trauma to the patella. However, it is more commonly associated with multiple factors including anatomical or biomechanical abnormalities and/or muscular weakness, imbalance and dysfunction. The orientation of the patella varies between individuals, it can also vary between left and right limbs in the same individual, which can result in anatomical malalignments that contribute to PFPS.

A common example of this imbalance is seen between two of the quadricep muscles. In many situations the Vastus Medialis Obliquus is weak in comparison to the Vastus Lateralis. This results in the Vastus Lateralis exerting a higher force on the patellofemoral joint and causes a lateral glide, tilt or rotation of the patella. This applies pressure on the lateral aspect of the femur. Repetitive pressure to this lateral aspect then leads to overuse of the area and eventually inflammation and pain of the lateral knee joint occurs.
Other Potential injury mechanics of PFPS:
- Tightness in the iliotibial band – which places excessive lateral force on the patella and can also externally rotate the tibia, altering the biomechanics of the patellofemoral mechanism.
- Tight hamstring muscles – Which applies posterior forces on the knee, causing pressure between the patella and the femur.
- Weakness of hip external rotators muscles – which results in compensatory foot pronation, again altering the tracking of the patella through changes in the tibia’s position in relation to the femur.
- Tight calf muscles – Which can lead to compensatory foot pronation (flat-footedness) and can increase the posterior force on the knee.
Signs and Symptoms:
In most cases, symptoms of patellofemoral pain syndrome develops gradually. Symptoms usually get worse with activity and may include:
- A dull, aching pain in the front of the affected knee, behind or close to the patella.
- Pain during activities that bend the knee, including squatting or climbing stairs (especially downstairs).
- Pain after sitting for extended periods of time where knees are kept bent.
- Crackling or popping sounds in the affected knee when standing up or climbing stairs.
- Pain that increases with sudden changes in regular playing surface, sports equipment or activity intensity.
Prognosis:
PFPS has no set time period for healing. It can become a long-term condition if left untreated as the mechanism which cause the injury do not tend to dissipate on their own; meaning the biomechanical insufficiency needs to be addressed. The longevity of the condition can often lead to greater levels of degeneration on the affected structures and eventually cause early onset arthritis or require surgical intervention. Therefore it is important to diagnose and treat this condition sooner rather than later.
What can your physiotherapist do for you?
Physiotherapists treat PFPS in a few ways. Firstly, they can loosen off of tight muscular structures such as the iliotibial band, hamstrings, quadriceps, hip external rotators and calf muscles through soft tissue massage, myofascial trigger point releases and superficial dry needling. This will help to alleviate painful symptoms which in turn can enable a larger range of motion for activities of daily living and strengthening exercises.

Secondly, they can prescribe exercise to help address the underlying biomechanical insufficiency. No only will this help to reduce immediate symptoms, it will also help to prevent PFPS returning in the future. Prescription of exercise is of significant importance when managing PFPS. Strengthening of the quadriceps is a key factor of PFPS rehabilitation (Bolgla & Malone 2005), in particular increasing the strength of the Vastus Medialis Obliquus has a positive effect on PFPS symptoms by increasing the medial forces projected onto the patella, counteracting the lateral shift of the patella. In addition to strengthening the quadriceps, it is important to strengthen the abductors and external rotators of the hip. Nakagawa et al 2008, found that increasing the muscle strength of certain muscle groups (quadriceps, abductors and external rotators of the hip) has a positive impact on PFPS symptoms. Furthermore, it has been recommended that eccentric strength training be implemented to the hip abductors in particular to treat PFPS. Eccentric strength training is the loading of a muscle whilst it is lengthening.

And lastly, in addition to strength training, Physiotherapists will also prescribe balance drills. Akseki et al 2008 & Clark et al 2000 agreed that the proprioceptive quality of PFPS patients was decreased. Proprioception is the perception or awareness of the position and movement of the body, which is a key component in the bodies ability to balance. Poor proprioceptive ability has been found to have direct correlation with other injuries such as anterior cruciate ligament injuries to the knee. Therefore it is a key factor in injury prevention for the affected knee.
If you have been experiencing knee pain on movement, and are worried PFPS may be occurring, contact your Physiotherapist for some timely advice!
- Bolgla L & Malone T, 2005. Research Review: Exercise Prescription and Patellofemoral Pain: Evidence for Rehabilitation.Journal of Sport Rehabilitation 14(1):72-88
- Nakagawa TH, Muniz TB, Baldon Rde M, Dias Maciel C, de Menezes Reiff RB, Serrão FV. The Effect of additional strengthening of hip abductor and lateral rotator muscles in patellofemoral pain syndrome: a randomized controlled pilot study. Clin Rehabil. 2008 Dec;22(12):1051-60. doi: 10.1177/0269215508095357.
- Akseki D, Akkaya G, Erduran M, Pinar H.Proprioception of the knee joint in patellofemoral pain syndrome. Acta Orthop Traumatol Turc. 2008 Nov-Dec;42(5):316-21.
- Clark DI, Downing N, Mitchell J, Coulson L, Syzpryt EP, Doherty M. Physiotherapy for anterior knee pain: a randomised controlled trial. Ann Rheum Dis 2000;59:700–704.

")

")
")